Mon 1 Dec 2014
Ozone during aluminum welding
Posted by admin under ACGIH, Air Monitoring, Chemical Exposure, Ethics, Exposure, Hazard Communication, hygienist, industrial hygienist, occupational hygiene, Ozone, PEL (Perm Exp Limit), Welding
Comments Off on Ozone during aluminum welding
Confession: I missed the assessment of this hazard the first time.
Awhile back I performed air sampling during aluminum welding. The welders were cordial and let me crawl over their welding equipment, poke around old boxes of wire and metal stock. I did not think there were any “real” hazards. We did find some airborne levels of various metals. From the picture can you tell who did the most welding?

After I had performed the sampling and the report was sent, I was asked if I had checked for ozone (O3)? I admitted I hadn’t and asked if it was an issue? Well, apparently it is (or rather, might be).
I went back to the shop, begged for another chance, and performed ozone sampling. It wasn’t difficult, but eating crow was the hardest part.
More information on the subject can be found at: NIOSH, UK- HSE. Ozone is formed when the UV radiation hits oxygen. The ACGIH TLV is variable (see table below)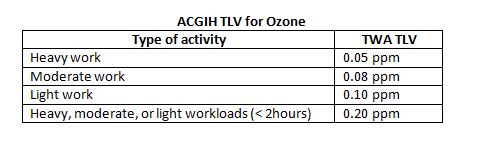 , and the OSHA PEL is 0.1 ppm.
, and the OSHA PEL is 0.1 ppm.
Health: Ozone, O3, can cause lots of different respiratory illnesses. These can include a decrease in lung function, aggravation of asthma, throat irritation/cough, chest pain, shortness of breath, inflammation of lungs, and a higher susceptibility to respiratory illnesses. ACGIH classifies it as an A4, or not a suspected carcinogen.
Luckily the results were found to be non-detectable (“IH talk” for none-found). Which only means I didn’t find it, not that it is not there. I sampled for a long time (530 minutes) because they were working 10 hour shifts. But, they only welded for a total of approximately 1.5 hours during that time.
If welders are in a confined area, or a small space with limited ventilation, the results might be significantly different.







